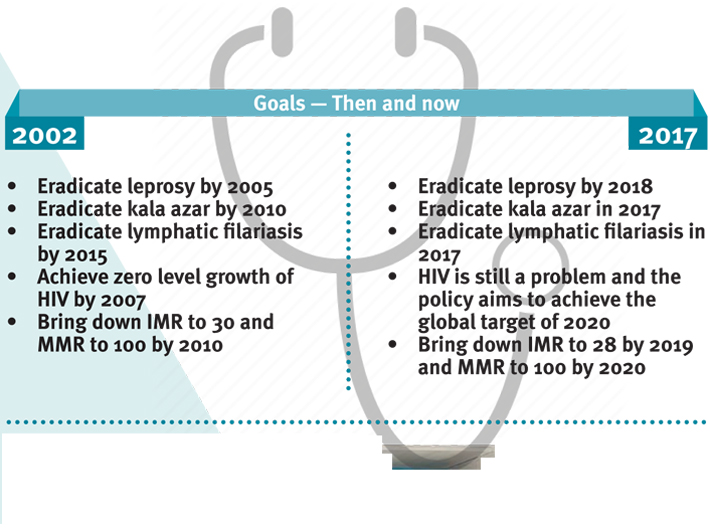
National Health Policy 2017 is nothing but a revision of the unmet targets of 2002 policy
GN Bureau | March 28, 2017

After much discussion and pondering over for more than two years, the cabinet has approved a new National Health Policy, scrapping the old one which was formulated in 2002. The government aims to increase the public health expenditure to 2.5% of the GDP by 2025. The policy formulated in 2002 aimed for reaching 2% of the GDP level by 2010. However, we hardly met our targets and the public funding on health remained around 1 to 1.15% since 2002. Described as the “huge milestone in the history of public health in the country” in an official press release, and “comprehensive and transformative,” by PM Narendra Modi, a comparative study with 2002 policy reveals that it has little new to offer.
Strengthening primary healthcare. But what’s new?
Patel: A Life By Rajmohan Gandhi Aleph Books, 568 pages, Rs 1,199 There are many biographi
The month of July exceeded its rainfall target despite forecasts of a below-normal month under a strengthening El Niño. The reason could be that climate change is amplifying monsoon complexity: West Pacific warming, Western Disturbances and evolving ocean conditions increasingly interact with El Ni&
Mumbai`s public space crisis is as much about mismanagement as it is about scarcity, and offers a governance roadmap that can be implemented without new legislation, according to a new report by the Urban Design Research Institute (UDRI) and the NGO Alliance for Governance and Renewal (NAGAR).
The Lok Sabha on Wednesday passed the Public Examinations (Prevention of Unfair Means) Amendment Bill, 2026 by a voice vote after an extensive discussion. Replying to the debate, minister of state (independent charge) for science & technology; earth sciences and MoS in the PMO, Dr. Jite
Shri Abhijit Phukon (IES: 2004) has been appointed as Joint Secretary, Department of Agriculture & Farmers Welfare, Government of India. His appointment, approved by the
Shri Avanish Kumar Mishra (ISS: 2000) has been appointed as Joint Secretary, Department of Administrative Reforms & Public Grievances (DARPG), Government of India. The appointment, approved by the Appointments













